
Infections
Medical and surgical management of eyelid and orbital infections — preseptal and orbital cellulitis, dacryocystitis, herpes zoster, and more.
Medically reviewed by Mark S. Brown, MDOculoplastic SurgeonLast updated June 2026
Blepharitis

Blepharitis is a chronic inflammation of the eyelid margins. It is one of the most common eyelid conditions and tends to recur despite treatment.
Blepharitis is usually inflammatory rather than infectious — chronic inflammation of the lid margins and meibomian glands (often with rosacea or Demodex), not a true infection. See the dedicated Blepharitis page for full detail.
Two Forms
- Anterior blepharitis affects the outer eyelid margin where the lashes attach. The most common causes are Staphylococcus aureus bacteria and seborrheic dermatitis. Patients develop crusting and collarettes at the base of the lashes.
- Posterior blepharitis (meibomian gland dysfunction) affects the inner lid margin. Obstruction of the oil-producing meibomian glands alters tear-film stability and leads to chronic dry-eye symptoms. Acne rosacea and seborrheic dermatitis are common co-existing conditions.
Symptoms
- Burning or stinging sensation, especially in the morning
- Crusty debris or collarettes at the base of the lashes on waking
- Intermittent blurred vision that improves with blinking
- Redness and thickening of the lid margin
- Foreign-body sensation and light sensitivity
Treatment
Daily lid hygiene is the cornerstone of management: warm compresses applied for five minutes soften meibomian-gland secretions, followed by gentle lid-margin scrubbing with a dilute baby-shampoo solution or commercial lid-scrub wipes. For moderate-to-severe disease, a course of oral doxycycline (50–100 mg daily for 6–12 weeks) is effective because of its anti-inflammatory effect on the meibomian glands, independent of its antibiotic properties.
Allergic Conjunctivitis
Allergic conjunctivitis is the most common allergic eye condition, affecting approximately 20% of the U.S. population. It results from IgE-mediated histamine release when the conjunctiva is exposed to an allergen.
Types
- Seasonal — triggered by outdoor pollen from trees, grasses, and weeds; symptoms peak in spring and fall.
- Perennial — caused by year-round indoor allergens such as dust mites, pet dander, and mold.
Symptoms
- Intense bilateral itching — the hallmark symptom
- Watery, red, and swollen eyes
- Eyelid swelling and mucous discharge
- Burning sensation and sensitivity to light
Management
First-line treatment is allergen avoidance combined with topical antihistamine/mast-cell stabilizer drops such as olopatadine (Pataday), which are effective and well tolerated. Systemic antihistamines and, in more severe cases, brief topical corticosteroid courses may be required under ophthalmic supervision.
Preseptal and Orbital Cellulitis
The orbital septum — a fibrous sheet running from the orbital rim to the tarsal plates — is the critical anatomic divider that determines the severity and management of periorbital infections.
Preseptal Cellulitis (Periorbital)
Infection confined to the eyelid and soft tissue anterior to the orbital septum. The globe and orbit are not involved: extraocular movements, pupil reactions, and visual acuity are normal.
- Most common in children, often following minor trauma, a skin infection, or an upper respiratory tract infection
- Common pathogens: Staphylococcus aureus and Streptococcus pyogenes
- Older children and adults may be managed as outpatients with oral antibiotics (amoxicillin-clavulanate)
- Children under five and any patient with worsening symptoms should be admitted for IV antibiotics and close monitoring
Orbital Cellulitis

Infection posterior to the orbital septum, involving the orbital fat and structures. Ninety percent of cases arise from direct extension of bacterial sinusitis. This is an ophthalmic emergency.
- Presents with fever, proptosis, painful restriction of eye movement, and decreased visual acuity
- An afferent pupillary defect, color-vision loss (dyschromatopsia), or rising intraocular pressure are signs of optic-nerve compromise that mandate urgent intervention
- CT scan of the orbit and sinuses is required to define the extent of infection and exclude abscess
- Hospitalization with broad-spectrum IV antibiotics is mandatory
- Failure to improve within 24–48 hours on IV antibiotics requires repeat CT and urgent surgical drainage
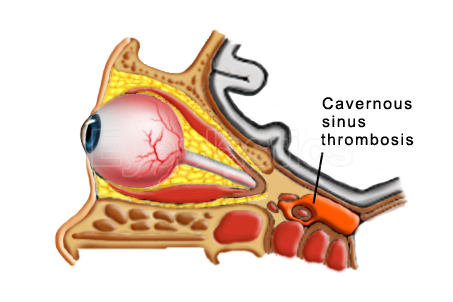
- Untreated orbital cellulitis can progress to orbital abscess, cavernous sinus thrombosis, meningitis, or permanent vision loss
Orbital cellulitis is a vision- and life-threatening emergency. Any patient with proptosis, restricted eye movement, or decreased vision requires urgent CT imaging and IV antibiotic therapy.
Herpes Zoster Ophthalmicus


Herpes zoster ophthalmicus (HZO) occurs when the varicella-zoster virus — dormant in the trigeminal ganglion after childhood chickenpox — reactivates and travels along the first division of the trigeminal nerve (V1), affecting the forehead, scalp, upper eyelid, and eye.
Risk Factors
- Incidence rises sharply after age 60
- Immunocompromised states (HIV, malignancy, immunosuppressive therapy)
- Physical or psychological stress
Clinical Features
- Prodromal pain, tingling, or burning in the V1 distribution, followed by a vesicular rash in a dermatomal pattern
- Hutchinson’s sign (vesicles at the nasal tip) predicts a higher likelihood of ocular involvement
- Ocular complications include keratitis, uveitis, eyelid scarring, corneal exposure, and ptosis
- Postherpetic neuralgia: persistent, often severe pain lasting months to years after rash resolution
Treatment
Oral antiviral therapy (acyclovir, valacyclovir, or famciclovir) should be started within 72 hours of rash onset to reduce severity, duration, and the risk of postherpetic neuralgia. Oculoplastic intervention may be required later to correct eyelid scarring, ectropion, or ptosis that results from cicatricial changes.
Prevention: The Shingrix vaccine (two doses) is recommended for all adults aged 50 and older, regardless of prior shingles history. It reduces the overall risk of shingles by roughly 90% and substantially lowers the risk of postherpetic neuralgia.
Lacrimal System Infections
Infections of the tear-drainage system — the lacrimal sac and canaliculi — are a distinct group of periorbital infections that often require surgical management for definitive cure.
Dacryocystitis
Dacryocystitis is infection of the lacrimal sac, caused by stasis of tears behind a blocked nasolacrimal duct. It presents as a painful, red, swollen mass at the inner corner of the lower eyelid.
- Acute dacryocystitis: Treated with oral or IV antibiotics (amoxicillin-clavulanate or cephalexin) and warm compresses. Pointing abscesses may require incision and drainage. Definitive treatment — dacryocystorhinostomy (DCR) — is planned after the acute infection subsides.
- Chronic dacryocystitis: Presents with recurrent tearing and mucopurulent discharge expressible from the lacrimal sac. DCR surgery creates a new drainage pathway directly into the nasal cavity and is the definitive treatment.
Canaliculitis
Canaliculitis is infection of the small tear-drainage channels (canaliculi) connecting the puncta to the lacrimal sac. It presents with redness, swelling, and yellow discharge at the inner corner of the eyelid.
- Most commonly caused by Actinomyces israelii, which forms characteristic yellow granular concretions (sulfur granules) within the canaliculus
- Treatment involves curettage to remove the concretions combined with topical antibiotic irrigation; penicillin drops are effective against Actinomyces
Frequently misdiagnosed. Because it mimics a persistent one-sided conjunctivitis, canaliculitis is often missed for months. See the dedicated Canaliculitis page for clinical photos, diagnosis, and the curative canaliculotomy with curettage.
Dacryoadenitis
Inflammation or infection of the lacrimal gland presents with tenderness and swelling of the outer upper eyelid. Viral causes include mumps, Epstein-Barr virus, and herpes zoster. Systemic conditions such as sarcoidosis, Sjögren’s syndrome, and lymphoma can produce a similar picture and must be excluded during evaluation.
Molluscum Contagiosum
Molluscum contagiosum is a common viral skin infection caused by the molluscum contagiosum virus (MCV), a DNA poxvirus. On the face and eyelids it produces characteristic small, flesh-colored, dome-shaped papules with a central dimple (umbilication).



Eyelid Involvement
When molluscum lesions involve the eyelid margin, viral particles shed into the tear film and trigger a chronic follicular conjunctivitis. The conjunctivitis will not resolve until the eyelid lesions are treated.
Who Is Affected
- Children aged 1–10 years (most common) through direct contact or shared towels and equipment
- Sexually active adults (genital or periocular spread)
- Immunocompromised individuals (HIV, transplant recipients) may develop extensive or atypical lesions
Treatment
- Curettage — mechanical removal under topical anesthesia; the most reliable approach for eyelid lesions
- Cryotherapy — light freeze with liquid nitrogen; effective but may cause transient depigmentation
- Expression — gentle trauma to express the central viral core; can be performed in the office
- Most lesions in healthy children resolve spontaneously within 6–18 months without intervention
Orbital Infections


The Chandler classification provides a clinically useful staging system for periorbital and orbital infections:
- Inflammatory edema — preseptal swelling without proptosis or restricted eye movement
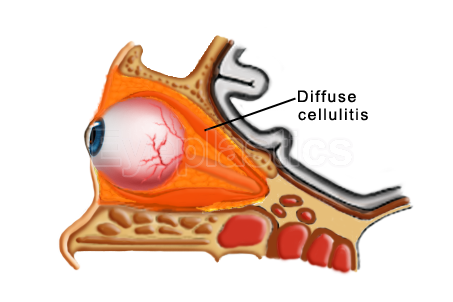
- Orbital cellulitis — diffuse post-septal infection without discrete abscess
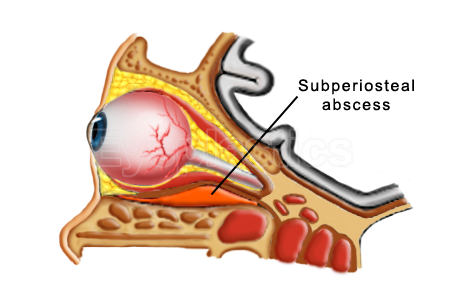
- Subperiosteal abscess — pus collection between the orbital wall and periorbita
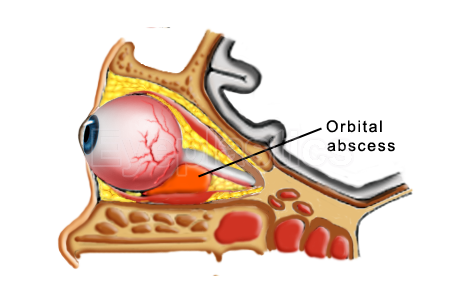
- Orbital abscess — abscess within the orbital fat itself
- Cavernous sinus thrombosis — intracranial extension; high morbidity and mortality
Orbital InfectionProgression (Chandler Stages)
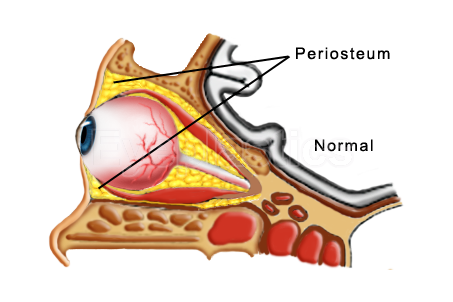
Step 1 of 5
Normal orbit — the orbital septum and periosteum keep the eye, fat and muscles compartmentalized.
Drag the slider to follow how an untreated orbital infection can progress through the Chandler stages.
Mucormycosis
Rhino-orbital-cerebral mucormycosis is a rare but rapidly fatal opportunistic fungal infection caused by fungi of the order Mucorales. It almost exclusively affects patients with poorly controlled diabetic ketoacidosis or severe immunocompromise.
- Infection begins in the paranasal sinuses and spreads aggressively into the orbit and cranial cavity
- The fungal hyphae cause vascular occlusion, producing black necrotic tissue — a hallmark clinical finding
- Treatment requires urgent surgical debridement (often including orbital exenteration), correction of the underlying metabolic abnormality, and systemic amphotericin B
- Hyperbaric oxygen therapy is used as an adjunct at some centers
Orbital Abscess
An orbital abscess is a collection of pus within the orbital fat, typically arising from untreated or inadequately treated orbital cellulitis (Chandler stage IV). It demands urgent surgical drainage to prevent permanent vision loss.
Subperiosteal Abscess
A subperiosteal abscess (SPA) forms between the bony orbital wall and the periorbita, most commonly on the medial wall from ethmoidal sinusitis. It is the most common orbital complication of sinusitis in children.
- A medial or inferior SPA may be drained via a transnasal endoscopic approach
- A superior SPA requires an external incision
Management Principles
- CT imaging to confirm abscess location, size, and extent before any surgical planning
- Failure to improve on IV antibiotics within 24–48 hours is a clear indication for surgical drainage
- Concurrent drainage of affected sinuses is performed at the same operation
- Prompt treatment is essential to prevent optic nerve compression, vascular compromise, and intracranial spread
Continue Reading — Complete Infection & Inflammation Guide
Frequently Asked Questions
- What is the difference between preseptal and orbital cellulitis?
- Preseptal cellulitis (periorbital cellulitis) is infection of the eyelid and tissues anterior to the orbital septum. It does not involve the orbit itself and is treated with oral antibiotics. Orbital cellulitis is a more serious infection posterior to the septum, involving the orbital fat and sometimes causing proptosis, pain with eye movement, and reduced vision — it requires IV antibiotics and often surgical drainage.
- What is dacryocystitis?
- Dacryocystitis is infection of the lacrimal sac, typically caused by nasolacrimal duct obstruction with secondary bacterial overgrowth. It presents as a painful, red, swollen mass at the inner corner of the eye. Acute dacryocystitis is treated with antibiotics; recurrent cases require DCR surgery to create a new drainage pathway.
- Can shingles affect the eye?
- Yes. Herpes zoster ophthalmicus (HZO) occurs when the varicella-zoster virus reactivates in the first division of the trigeminal nerve, affecting the forehead, scalp, and eye. It can cause eyelid scarring, corneal disease, and ptosis. Treatment includes antiviral medications and may require oculoplastic intervention for eyelid complications.
- When should I see an oculoplastic surgeon for an eyelid or orbital infection?
- You should seek immediate care from an oculoplastic surgeon if you experience severe eye pain, vision changes, fever, or rapidly spreading redness and swelling around the eye, as these may indicate a serious infection requiring specialist evaluation. Additionally, if you have recurrent infections, complications from previous infections, or infections that don't improve with antibiotics prescribed by your primary care doctor, an oculoplastic surgeon can provide advanced diagnostic imaging and specialized treatment. Your primary care physician or ophthalmologist can refer you to a fellowship-trained oculoplastic surgeon when needed.
- What happens during a consultation for an eyelid or orbital infection?
- During your consultation, the oculoplastic surgeon will perform a detailed examination of your eye, eyelid, and surrounding tissues, and may order imaging studies such as CT or MRI scans to assess the extent and location of the infection. They will review your symptoms, medical history, and any prior treatments you've received to determine whether medical management (antibiotics), surgical drainage, or another intervention is appropriate. The surgeon will discuss the findings with you and create a treatment plan tailored to your specific situation.
- What is the typical recovery process after treatment for an orbital infection?
- Recovery depends on the severity of your infection and the type of treatment received; patients with preseptal cellulitis treated with antibiotics may improve within days to a week, while those requiring surgical drainage typically recover over several weeks. Most patients can return to normal activities gradually as swelling decreases and infection clears, though strenuous exercise should be avoided during the acute phase. Dr. Brown will provide specific post-operative instructions, including when to resume work and normal routines, and will schedule follow-up visits to ensure proper healing.
- What are the potential complications if an orbital infection is not treated promptly?
- Untreated orbital infections can lead to serious complications including vision loss, abscess formation, meningitis, sepsis, and in rare cases, permanent damage to eye muscles or the optic nerve. Prompt recognition and treatment are crucial to prevent these outcomes and preserve your vision and eye health. If you suspect an orbital infection, seek immediate medical attention rather than waiting to see if symptoms improve on their own.
Ready to discuss Infections?
Schedule a consultation with Mark S. Brown, MD to learn if this procedure is right for you.