

Demodex Blepharitis
Eyelash-mite infestation (Demodex folliculorum & brevis) — the cause of collarettes, chronic lid irritation, and a common driver of blepharitis, MGD, and dry eye.
Medically reviewed by Mark S. Brown, MDOculoplastic SurgeonLast updated June 2026
What is Demodex Blepharitis
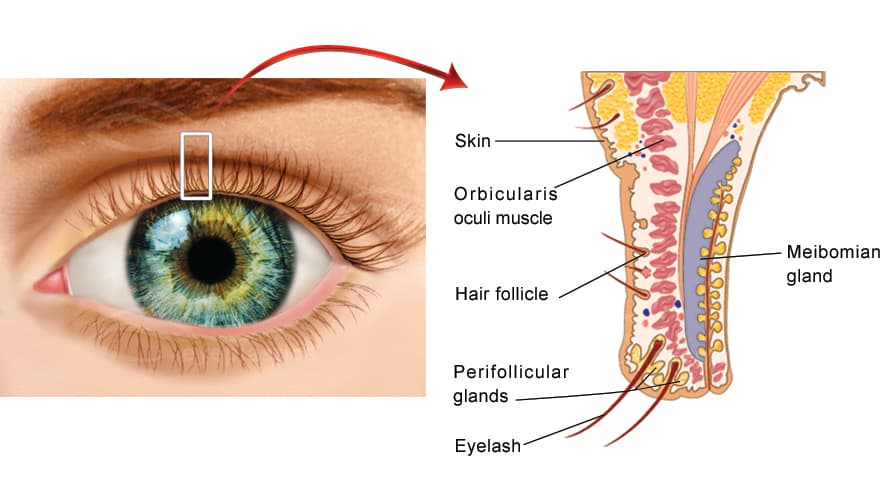
Demodex blepharitis is a chronic inflammation of the eyelid margins caused by an overpopulation of microscopic Demodex mites that live in and around the eyelash follicles and the oil (meibomian) glands of the lids. It is one of the most common — and most frequently missed — causes of blepharitis. Mites are a normal resident of human skin, but when their numbers rise they trigger lid-margin irritation, the characteristic waxy debris called collarettes, and a cycle of itching, redness, and tear-film instability.
This page is the in-depth companion to our main Blepharitis guide. Demodex overlaps heavily with meibomian gland dysfunction (MGD), dry eye disease, and ocular rosacea — the conditions are often treated together.
The Two Mites Behind the Disease
Two related species cause ocular Demodex disease, and they tend to produce two different patterns of blepharitis:
Demodex folliculorum
Lives inside the eyelash follicle, usually in clusters around the lash root.
- Drives anterior blepharitis
- Produces the cylindrical collarettes wrapped around the lash base
- Associated with lash misdirection, lash loss, and recurrent irritation
Because the two species occupy different parts of the lid, many patients have a mixed picture — anterior collarettes and meibomian gland obstruction — which is why Demodex is so often intertwined with dry eye and MGD.
Collarettes — The Telltale Sign
Collarettes — sometimes called cylindrical dandruff — are translucent, waxy cuffs of mite waste and skin debris that form a clear sleeve around the base of the eyelashes. They are considered pathognomonic for Demodex: if a patient has collarettes, they have Demodex blepharitis. Unlike the hard, brittle scales (scurf) of staphylococcal blepharitis, collarettes are soft, semi-clear, and slide up the lash as it grows.
Clinical pearl: Collarettes are best seen by asking the patient to look down while examining the upper lid lashes at the slit lamp. Their presence and number are now used to grade disease severity and to track response to treatment.
Who Gets It
Demodex colonization rises steadily with age — it is nearly universal in the elderly — but symptomatic disease can occur at any age. Recognized associations include:
- Older age — the single strongest risk factor
- Facial and ocular rosacea — strongly linked to Demodex overgrowth
- Chronic blepharitis, MGD, and dry eye that has not responded to standard lid hygiene
- Recurrent chalazia or styes
- Oily skin (seborrhea), diabetes, and immune compromise
- Long-term contact lens wear and incomplete eye-makeup removal
Symptoms
- Itching of the eyelid margins — often the dominant complaint, classically worse in the morning
- Burning, foreign-body or gritty sensation
- Red, irritated, crusted lid margins with debris at the lash bases
- Watery eyes alternating with dryness and fluctuating, blink-dependent blurred vision
- Lashes that feel sticky, brittle, misdirected, or that fall out (madarosis)
- Recurrent chalazia and a feeling that "nothing the patient tries fully works"
Ready to discuss Demodex Blepharitis?
Schedule a consultation with Mark S. Brown, MD to learn if this procedure is right for you.